CHC Funding: A Caregiver’s Step-by-Step Guide (2026) | Care Sync Experts Blog | Care Sync Experts
CHC Funding: A Caregiver’s Step-by-Step Guide (2026)
Text to speech
00:00
5sec
Duration: 00:00
Font size
Published: 26 Feb, 2026
Share this on:
CHC funding (NHS Continuing Healthcare funding) is a free, non-means-tested package of care that the NHS fully funds for adults with complex, intense, or unpredictable long-term health needs. If someone has a primary health need, the NHS pays for their care in full, whether that care takes place at home, in a nursing home, or in another community setting.
To qualify, the NHS first completes a CHC Checklist and, if needed, carries out a full CHC assessment using a multidisciplinary team and Decision Support Tool.
Spot CHC Early: The Caregiver Signs That Trigger an Assessment
As a caregiver, you often notice the warning signs before anyone else. If care feels more medical than social, you should consider raising CHC funding with the NHS.
You should request a CHC Checklist if the person you support:
Needs frequent clinical intervention (complex wound care, PEG feeding, oxygen therapy, or specialist medication management)
Faces unpredictable risks such as seizures, choking, falls, or sudden deterioration
Requires constant supervision to prevent harm
Has behaviour, cognition, or psychological needs that demand skilled monitoring
Shows rapid decline, especially in late-stage or life-limiting conditions
CHC does not depend on diagnosis, income, savings, or property ownership. It depends on whether the person’s needs revolve around managing health risks rather than providing routine social care.
If you believe health needs drive the care plan, do not wait for someone else to raise it. Ask the GP, district nurse, hospital discharge team, or social worker to start the NHS Continuing Healthcare checklist process.
CHC Guidance in One Rule: Health Needs Decide, Not Money
The core rule behind CHC funding is simple: the NHS looks at health needs, not bank accounts.
You qualify for continuing healthcare if your overall needs show a primary health need. This means your care mainly addresses medical risks and clinical complexity, rather than routine support with daily living.
During a CHC assessment, decision-makers examine four key characteristics:
Nature – What type of health needs exist?
Intensity – How much care is required, and how often?
Complexity – How do different conditions interact and increase risk?
Unpredictability – How likely is sudden deterioration or harm without skilled oversight?
For example, help with washing and dressing alone does not usually trigger CHC funding. But if that same person also faces unstable blood sugar, high infection risk, behavioural risks, and frequent medication changes, the picture shifts from social care to healthcare.
As a caregiver, your role is to frame needs clearly. Describe what happens when care does not go right. Document risks, frequency, and consequences. The NHS does not fund diagnoses, it funds risk, intensity, and complexity.
That is the foundation of all CHC guidance and the CHC framework.
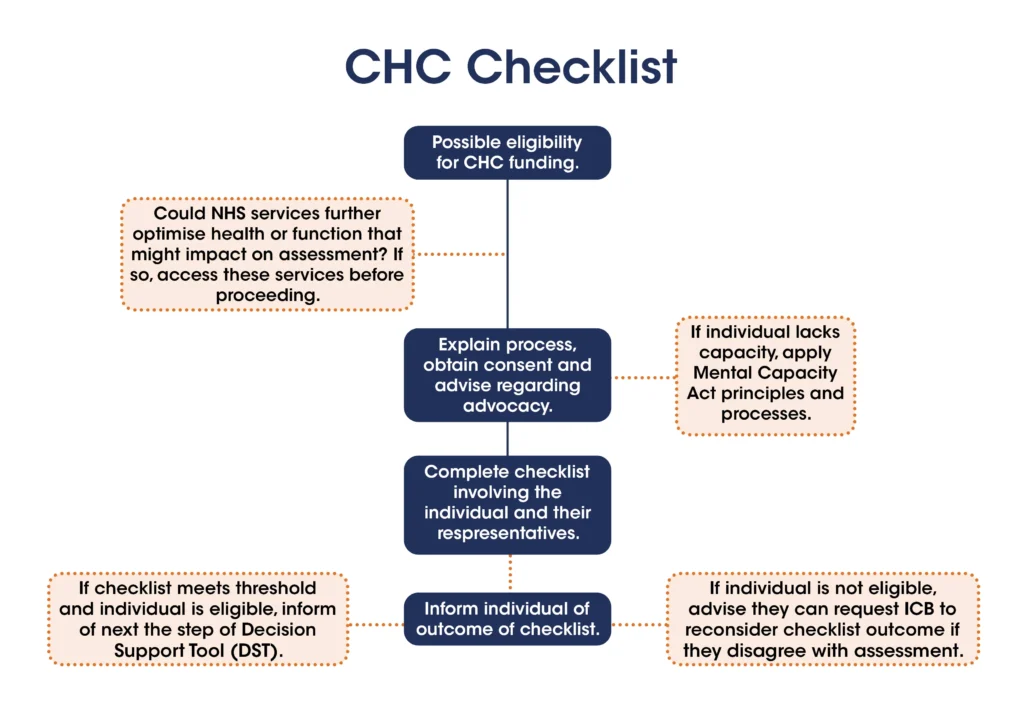
Start With the CHC Checklist (NHS Continuing Healthcare Checklist)
The CHC Checklist acts as the screening stage for CHC funding. A nurse, GP, hospital clinician, or social worker completes it to decide whether the person should move to a full CHC assessment.
The NHS Continuing Healthcare checklist does not decide eligibility. It simply asks: “Does this person need a full assessment?”
You should always:
Confirm that a trained professional completes the Checklist
Ask for a copy of the completed document
Request written reasons for the outcome
Check that the recorded needs reflect reality
If the Checklist shows sufficient need, the NHS must arrange a full assessment. If it does not, you can challenge the outcome and ask for reconsideration.
Caregiver Move: Bring Evidence to the Checklist
Do not attend empty-handed. The Checklist works best when you support it with clear, recent evidence:
Daily care notes showing frequency of intervention
Avoid vague descriptions like “needs a lot of support.” Instead, say:
“Requires repositioning every two hours due to Grade 3 pressure ulcer risk. Missed repositioning led to skin breakdown on 12/02.”
The Checklist stage sets the tone for everything that follows. If you document intensity and risk early, you strengthen your case before the full CHC assessment even begins.
Prepare for the Full CHC Assessment Like an Inspection
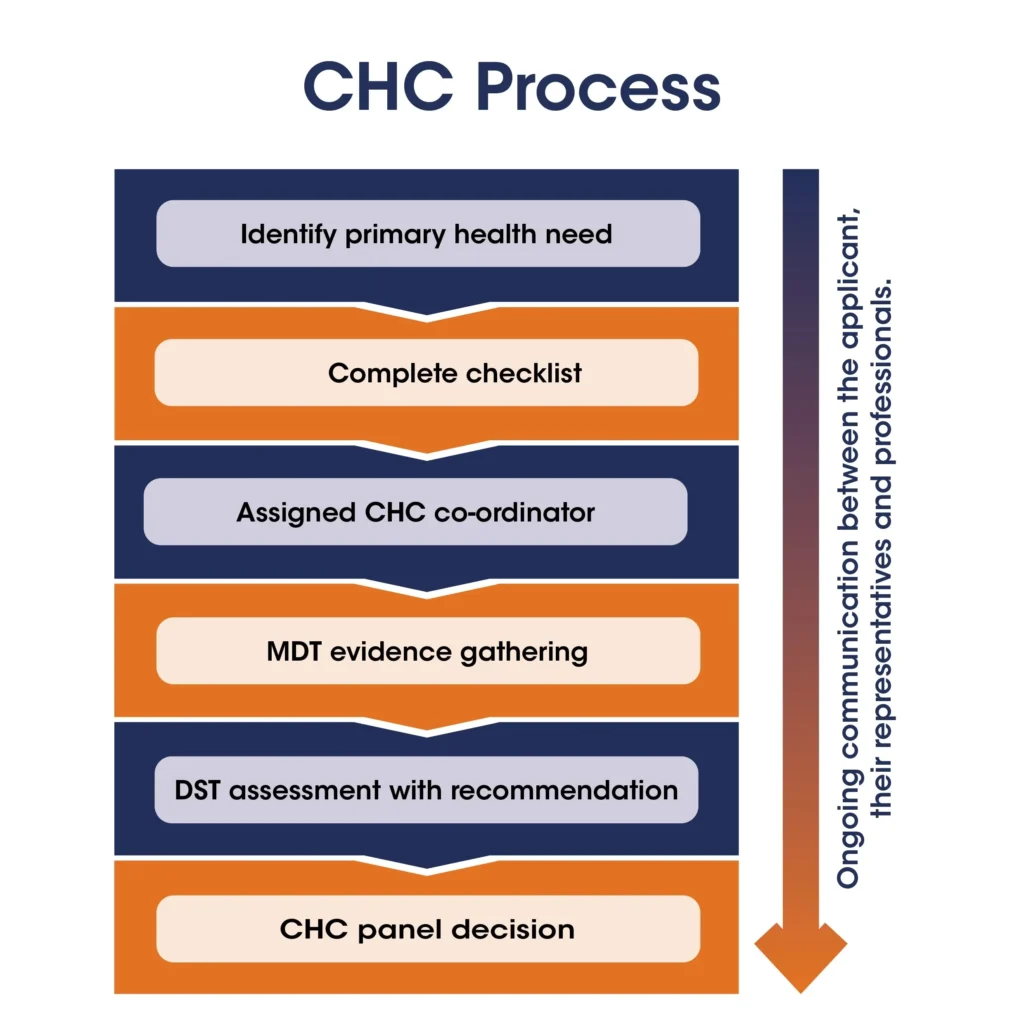
CHC Funding- Process
If the CHC Checklist triggers a full review, the NHS arranges a CHC assessment led by a multidisciplinary team (MDT). This team usually includes at least two professionals from different disciplines, often health and social care staff already involved in the person’s care.
The MDT uses a document called the Decision Support Tool (DST). It breaks needs into care domains such as mobility, nutrition, cognition, behaviour, skin integrity, breathing, medication, and more. Each domain receives a level: priority, severe, high, moderate, low, or no need.
But levels alone do not decide CHC funding. The MDT must also judge how the needs combine under the four key tests:
Intensity – How much care does the person require daily?
Complexity – How do multiple conditions interact?
Unpredictability – How often does risk escalate suddenly?
Nature – What kind of clinical skill does safe care demand?
Caregiver Strategy: Link Evidence to Each Domain
Do not rely on professionals to “know the story.” Prepare a short summary that maps evidence to domains.
For example:
Skin: Grade 3 pressure ulcer history; repositioning every 2 hours; district nurse involvement.
Medication: Frequent dosage changes; risk of hypoglycaemia; nurse oversight required.
Behaviour: Verbal aggression during personal care; requires two carers to prevent harm.
Focus on risk, consequences, and frequency. Show what happens when support fails.
When you present needs clearly and in active terms, you help the MDT see the full picture, not isolated tasks, but an interconnected health risk profile.
Use Fast Track When the Condition Deteriorates Rapidly
When someone’s health declines quickly, and professionals believe they may be approaching the end of life, you do not need to wait for the standard CHC assessment process. The NHS can activate the Fast Track pathway.
Fast Track allows the NHS to arrange CHC funding immediately, without completing the full Checklist and Decision Support Tool first. A clinician, usually a GP, consultant, or specialist nurse, completes a Fast Track tool confirming rapid deterioration.
As a caregiver, you should raise Fast Track if you notice:
Clear clinical decline over weeks or days
Escalating symptoms that require skilled intervention
Frequent hospital admissions or crisis events
End-of-life indicators
Do not assume someone else will suggest it. Ask directly: “Does this situation meet the criteria for Fast Track CHC?”
Fast Track exists to remove delay during urgent periods. If the clinical team agrees that deterioration is significant, the NHS should arrange a funded care package quickly so care remains stable and dignified.
Track the CHC Timeline: Know the 28-Day Expectation
CHC Funding
Once someone requests a full CHC assessment, the local Integrated Care Board (ICB) should normally complete the decision within 28 days of receiving a completed Checklist or request for full assessment.
This timeframe matters. Delays create stress, financial pressure, and uncertainty for families and caregivers.
As a caregiver, take control of the timeline:
Record the date the CHC Checklist was completed
Record the date of referral for full assessment
Record the MDT meeting date
Record when the ICB issues its decision letter
If the ICB decides the person qualifies for CHC funding but takes longer than 28 days without justified reason, it may need to refund care costs from day 29 onward.
Keep communication written wherever possible. Confirm conversations by email. A simple timeline log strengthens your position if you need to challenge delays.
When you monitor the process closely, you reduce the risk of administrative drift and protect the person’s entitlement to continuing healthcare.
Challenge a CHC Decision With Evidence, Not Emotion
If the NHS refuses CHC funding, do not treat the decision as final. Many families secure eligibility after challenging weak reasoning or incomplete assessments.
Start by requesting:
A full copy of the Decision Support Tool (DST)
The written rationale explaining why the person does not have a primary health need
Copies of any risk assessments used
Read the document carefully. Look for gaps. Did the MDT downplay intensity? Did it ignore unpredictable risks? Did it describe health needs as “social care” without explaining why?
Caregiver Strategy: Reframe the Case Clearly
When you challenge a decision, respond domain by domain. Link each disagreement to evidence.
For example:
“The DST records mobility as moderate. However, records show two falls requiring hospital review within three weeks.”
“Medication management involves insulin titration with risk of hypoglycaemia. This reflects clinical intensity, not routine support.”
You can ask the ICB to reconsider its decision locally. If dissatisfaction continues, you may request an independent review through the NHS complaints route.
Focus on documented risk, frequency, and consequences. Avoid emotional language. Clear evidence carries more weight than frustration.
A refused decision does not mean the person lacks needs. It often means the evidence did not fully demonstrate the health risk profile at that time.
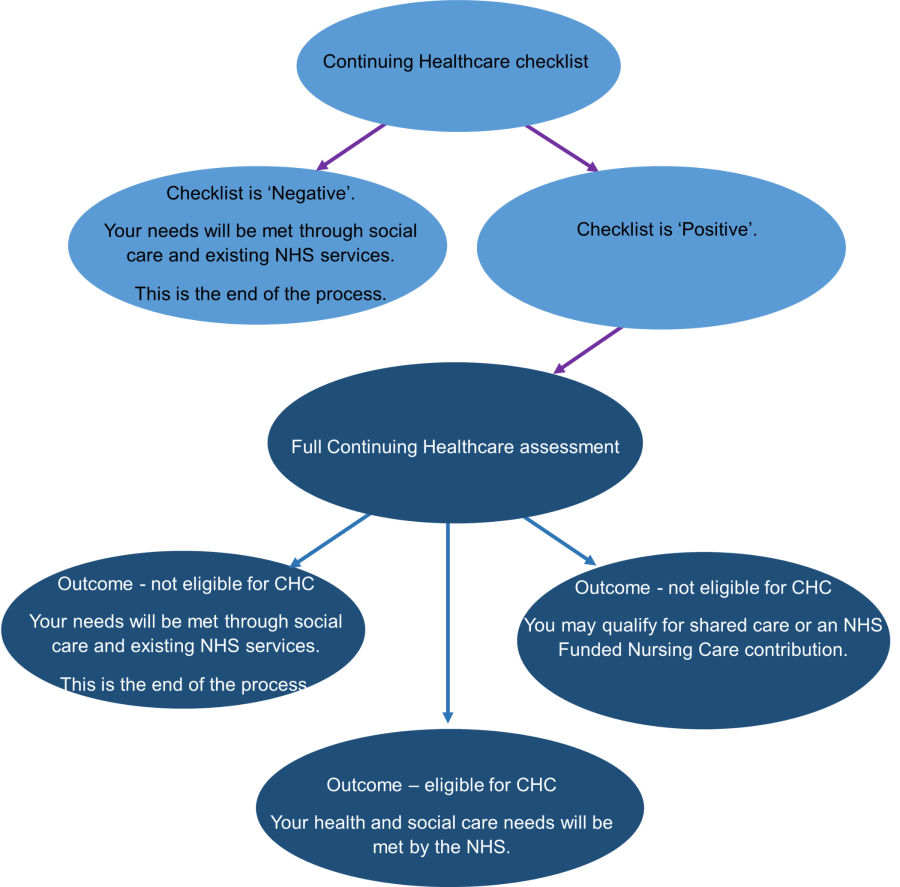
If CHC Funding Fails, Check FNC Funding
NHS Continuing Healthcare for Adults
If the NHS refuses CHC funding, you should immediately check eligibility for FNC funding (NHS-funded nursing care).
FNC funding applies when someone lives in a nursing home and requires support from a registered nurse, but does not meet the threshold for full continuing healthcare. Instead of paying the entire care package, the NHS pays a set weekly contribution toward the nursing element of care. The individual or local authority covers the remaining costs.
You do not usually need a separate assessment for FNC if the person has already completed a full CHC assessment. The MDT should consider FNC automatically during that process.
As a caregiver, confirm:
The home is registered to provide nursing care
The assessment clearly identifies ongoing nursing needs
The ICB confirms the FNC rate and payment arrangement
FNC funding does not replace CHC, but it can reduce financial pressure if full eligibility does not apply. Always ask for written confirmation of the decision and review dates, as nursing needs should be reviewed regularly.
If you want to start or chase a CHC assessment, contact your local Integrated Care Board (ICB). The ICB manages CHC funding decisions in your area.
You can:
Ask your GP, district nurse, hospital discharge team, or social worker to submit a referral
Call your local ICB and request the CHC team directly
Ask for the named CHC case coordinator handling the case
When you call, stay clear and direct: “I would like to request a CHC Checklist for [name]. Their needs involve complex health risks, and I believe they may have a primary health need.”
If you need independent guidance, the organisation Beacon offers free advice on continuing healthcare. They operate a helpline and can explain next steps without charging families.
Always follow up phone calls with an email. Written records protect you if delays occur.
Taking early control of communication often speeds up the CHC funding process and prevents your case from stalling in the system.
If You Are Paying While Waiting: Ask About Short-Term Support
If the NHS delays a CHC funding decision and care costs continue, do not ignore temporary support options.
Local councils run emergency cost-of-living schemes under the Household Support Fund. This fund helps residents who face immediate financial hardship with essential costs such as utilities, food, and basic household items. Each council manages its own household support fund application, so eligibility and payment rules vary by area.
If you need help urgently, search your council website for “household support fund apply online” or contact the council’s welfare support team directly. They will explain whether you qualify and how to submit a household support fund application.
This support does not replace continuing healthcare, and it does not affect your CHC assessment. It simply provides short-term relief while funding decisions progress.
Always keep receipts and records of payments made during the waiting period. If the NHS later confirms CHC eligibility, you may need documentation if reimbursement discussions arise.
Final Checklist for Caregivers: Take Control of the CHC Process
Before you close this guide, use this quick action list to stay ahead of the CHC funding process:
Request the CHC Checklist as soon as health needs escalate
Map evidence to intensity, complexity, unpredictability, and nature
Track every date in the CHC assessment timeline
Ask for written decisions and full documentation
Challenge weak reasoning with structured evidence
Check FNC funding if full eligibility does not apply
Contact your local ICB directly if communication stalls
You do not need to become a legal expert to secure continuing healthcare. You need structured evidence, clear communication, and persistence.
When you focus on health risk rather than tasks, document frequency rather than general need, and stay proactive at each stage, you place yourself in the strongest position to secure the right outcome.
Need Help Securing CHC Funding?
If you feel overwhelmed by the CHC assessment process or want expert support before, during, or after a decision, Care Sync Experts can guide you step by step.
We help caregivers and care providers:
Prepare strong evidence before the CHC Checklist
Structure cases clearly for the full CHC assessment
Challenge refusals with documented, domain-based responses
Navigate appeals professionally and strategically
CHC decisions should reflect real health risks, not paperwork gaps.
Yes. The NHS can withdraw CHC funding if a review shows that the person no longer has a primary health need.
Integrated Care Boards (ICBs) must review CHC packages after three months and then at least annually. If needs reduce in intensity, complexity, or unpredictability, the NHS may decide that full continuing healthcare no longer applies.
If funding is withdrawn, you have the right to: – Request a written explanation – Challenge the decision – Provide updated evidence – Ask for a reassessment if needs change again
CHC is based on current needs. If those needs increase later, you can request a new assessment.
What Are the 4 Criteria for CHC?
The NHS decides eligibility using four characteristics: – Nature – What type of health needs exist? – Intensity – How much care is required and how often? – Complexity – How multiple conditions interact and increase risk – Unpredictability – The likelihood of sudden deterioration or harm
Decision-makers apply these criteria during the full CHC assessment when determining whether someone has a primary health need.
Is There a Limit to CHC Funding?
No. There is no financial cap on CHC funding. If someone qualifies, the NHS must cover the full cost of meeting assessed health and associated care needs. This applies whether care takes place at home or in a care home.
The NHS can consider value for money when arranging a package, but it cannot refuse funding simply because care is expensive if the person meets eligibility criteria.
What Is the Full Form of CHC in Medical Terms?
CHC stands for Continuing Healthcare. In England, the formal term is NHS Continuing Healthcare, which refers to a fully funded package of care for adults with complex or long-term health needs.
It is sometimes shortened to “CHC funding” when referring to the financial aspect of the package.